



Tracheal intubation is a medical procedure in which a flexible tube is inserted into the trachea.
Tracheal tubes vary in size and design for different patients with cuffs help aspiration prevention and ensure good ventilation.
Direct laryngoscopy is used as a traditional method in which a laryngoscope sees vocal cords for intubation.
Procedure conducted using direct or video laryngoscopy guidance and selection of technique are based on clinical scenario and anatomy of patient.
- Laryngoscope
- Endotracheal Tubes
- Stylet
- Suction Apparatus
- End-tidal Carbon Dioxide Monitoring
- Oropharyngeal and Nasopharyngeal Airway Devices
Informed Consent:
The procedure should be thoroughly discussed with the patient, to ensure informed consent.
Patient Positioning:
Place patient in optimal airway alignment, usually with head in sniffing position for vocal cord visualization.
Step 1: Anesthesia
Inject sedatives as anesthesia for relaxing muscles. Before this ensure proper supply of oxygen for patient during intubation.
Step 2: Vocal Cord Visualization
The surgeon inserted laryngoscope in mouth, then slowly displaced to see the epiglottis.
Lift epiglottis to expose vocal cords for visualization.
Step 3: Tube insertion
Insert endotracheal tube through mouth along tongue curve then guide towards glottis.
Use correct air volume of cuff endotracheal tube to prevent aspiration.
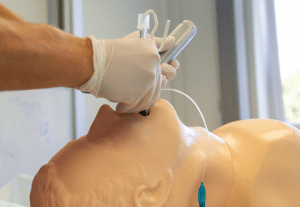
Fig. Anterior neck view
Step 4: Confirmation
Confirm proper endotracheal tube placement with help of chest X-ray and listening stable breath sounds.
Intubation has risks of introducing pathogens, which increase pneumonia in respiratory patients.
Misuse of laryngoscope blade and endotracheal tube insertion may damage larynx and trachea.
Misplacement of endotracheal tube can lead to insufficient breathing support.
Incorrect tube placement or cuff inflation can lead to gastric aspiration.
LEARNING & CME
View All
Advanced
Cardiovascular
Life Support

Basic Life
Support

Pediatric
Advanced Life
Support

Neonatal
Resuscitation
Program

Annual Stroke
Center
Continuing
Education

Opioid and Pain
Management

National
Institutes of
Health Stroke
Scale

Basics of
Electrocardiography