



Plasmapheresis term also include therapeutic plasma exchange (TPE) and is a medical procedure in which plasma is removed from the blood. Blood plasma is the liquid portion of blood and includes water; electrolytes; hormones; and proteins; some of which are antibodies. This process is routinely used for treatment of many autoimmune diseases, neurological disorders and some other hematological disorders, wherein the harmful substances produced by the body are selectively separated from the blood.
Plasmapheresis
Plasmapheresis term also include therapeutic plasma exchange (TPE) and is a medical procedure in which plasma is removed from the blood. Blood plasma is the liquid portion of blood and includes water; electrolytes; hormones; and proteins; some of which are antibodies. This process is routinely used for treatment of many autoimmune diseases, neurological disorders and some other hematological disorders, wherein the harmful substances produced by the body are selectively separated from the blood.
Plasmapheresis
Myasthenia Gravis: There are high levels of circulating antibodies against acetylcholine receptors that depress the muscle during the crisis.
Guillain-Barré Syndrome (GBS): Proven in helping to lessen the disease’s effect and in promoting faster healing.
Systemic Lupus Erythematosus (SLE): Used in severe conditions, especially when complication such as nephritis or central nervous system is involved.
Vasculitis: Particularly in cases like anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis.
Multiple Sclerosis: In severe worsening (especially in the case of relapsing form) to cleanse the body of antibodies and inflammatory agents.
Thrombotic Thrombocytopenic Purpura (TTP): Essential for rapidly removing large von Willebrand factor multimers and inhibiting platelet aggregation.
Severe Hypotension: Patients with significantly low blood pressure could not cope well with the procedure.
Coagulopathy: Patients with bleeding disorders or thrombocytopenic patients are vulnerable to develop hemorrhage during or after the operation.
Severe Infection: There are likely to be more active infections post the procedure since immunocompromised patients may be vulnerable to infections.
Heart Failure: Volume changes can be particularly dangerous in patients with congestive heart failure or high probabilities of severe cardiac dysfunction.
Allergic Reactions: Contraindications include history of severe adverse reactions to apheresis products or replacement solutions.
Apheresis Machine
Blood Collection Sets
Plasma Collection Bags
Anticoagulants
Monitoring Equipment
Return System
Control Software
Patient preparation
Pre-Procedure Assessment
Medical History: Check the patient’s medical history particular diseases that may be chronic, drug allergies and any medications they may be taking.
Indication for Plasmapheresis: Enquire and establish the cause of the procedure (for example, autoimmune diseases, renal diseases and the rest).
Laboratory Tests
CBC, electrolyte and coagulation studies should be done to determine baseline values before starting the treatment.
Immunoglobulin Levels: If possible, test for immunoglobulins.
Patient Education
Explain the Procedure: Explain what exactly happens in plasmapheresis, how long it should take, the possible negative effects and the positive results that may be derived there from.
Address Concerns: Make sure to address the patient questions and that you reassure them if they have any concerns.
Informed consent: Take informed consent from the patient.
Pre-Medication
Medications: Administer pre-medication before surgery where necessary or as per physician’s order (e.g., antihistamine, corticosteroids as an allergic prophylactic measures).
Equipment Set Up Monitoring: Ensure that the equipment needed for continuous observation of additional measures, such as vital signs like heart rate, blood pressure, and oxygen saturation, is available.
Step 1-Patient Preparation Assessment:
The clinical state and previous pathologic history of the patient and the reasons for plasmapheresis are evaluated.
Some people experiencing the following conditions present signs suggestive of the condition, they include autoimmune diseases such as Guillain-Barré syndrome, myasthenia gravis, hyper viscosity syndrome or certain blood disorders.
Informed Consent: The patient is explained the procedure including potential complications and possible advantages.
IV Access:
Vascular access must be established.
A large-bore peripheral IV catheter may be sufficient for short-term treatment; however, a central venous catheter (CVC) or dialysis catheter is typically implanted for repeated sessions.
Baseline Monitoring: A pulse and oxygen saturation rate are measured, and the patient’s blood pressure is taken. Some of the blood tests are CBC, clotting profile and electrolyte panel.
Step 2-Priming the Machine:
Plasmapheresis Device Setup: A plasmapheresis machine is prepared and primed with a sterile solution (usually saline) to ensure that air is removed from the circuit.
Anticoagulation: Since many procedures require arterial line draws, anticoagulants such as heparin or citrate are used and pumped into the system to stop blood clotting during the process.
Blood Withdrawal: A sample is collected from the patient using the IV or central catheter to introduce fluids into the patients’ bloodstream. The blood is then entered into the plasmapheresis machine that filters its components.
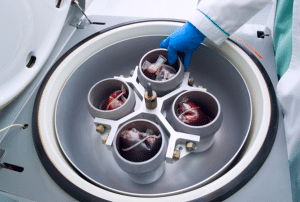
Plasma Separation Centrifugation or Filtration: The machine then separates the component of the blood using a centrifuge or using a filter.
Centrifugation: Blood is whirled rapidly in a centrifuge or centrifuged to isolate plasma and narrow down it to red blood cells (RBCs), white blood cells (WBCs) and platelets.
Filtration: Blood is pumped through a filter, while plasma can freely pass through the filter membrane because of the holes while blood cells cannot pass through it. The separated plasma thereafter is either disposed or processed based on the conditions being treated.
Step 3-Replacement of Plasma:
The removed plasma is replaced with a replacement. Fluids that can be used as replacements for the purpose are:
Fresh frozen plasma (FFP): In the event that coagulation factors need to be replenished.
Albumin solution: The most common volume expander.
Saline: Its use can be very occasional, most often combined with albumin.
The replacement fluid is given to the patient in ways that provide fluid balance and hemodynamic stability.
Step 4-Reinfusion of Blood Cells:
The remaining components of the blood referred to as blood components (RBCs, WBCs, and platelets) get returned to the patient through the same catheter.
This reinfusion makes sure the patient has enough of the cellular blood components and avoid situations where a patient develops anemia or thrombocytopenia.
Step 5-Monitoring During the Procedure:
Vital Signs: The patient’s heart rate, blood pressure, and oxygen levels are closely monitored throughout the process to detect any adverse effects, such as hypotension or allergic reactions.
Calcium Monitoring: Since citrate complexes with calcium, patients may sometimes develop hypocalcemia or low levels of calcium of in the blood.
Oral or intravenous calcium therapy is usually prescribed during or after the procedure to counter feelings of numbness or muscle twitching.
Anticoagulation Monitoring: Vigilance for the onset of bleeding is important since anticoagulants are used.
Step 6-Completion of the Procedure:
The procedure ends after a specified plasma volume is taken out and replaced (total plasma volume for the patient, usually it is 1 to 1.5 times).
The IV or central catheter is rinsed with saline; anticoagulants are titrated.
The machine is also washed and disinfected in a prescribed manner. Post-procedure Care
Vital Sign Monitoring: Depending on the type of procedure that has been performed the patient goes through monitoring of their vital signs for some time after the procedure.
Lab Tests: Blood tests are repeated to determine levels of electrolytes, coagulation status, and hematocrit.
Side Effects Observation: The side effects are monitored in the patient; the manifestations include:
Hypotension: Caused by fluid shifts.
Allergic Reactions: If fresh frozen plasma is used.
Hypocalcemia: As associated with citrate anticoagulation.
Fluid and Electrolyte Management: Abnormalities of serum concentrations from calcium to potassium are treated when necessary.
Complications
Hypotension: A drop in blood pressure can occur, particularly during the procedure, due to fluid shifts and loss of plasma volume.
Allergic Reactions: Post procedural complications may include reactions to the anticoagulants, or the replacement solution administered during the procedure.
Infections: Infection of the access site is always possible; this is so especially if one is using a central venous catheter.
Thrombosis: It is also seen that blood clot formation is likely to happen in the access vein where good anticoagulation may not be done all the time.
Electrolyte Imbalances: Plasma depletion may upset the normal electrolyte concentrations in the body hence resulting to hypocalcalemia.
Hypoproteinemia: A decrease in plasma protein levels can occur, potentially leading to edema and other issues.
LEARNING & CME
View All
Advanced
Cardiovascular
Life Support

Basic Life
Support

Pediatric
Advanced Life
Support

Neonatal
Resuscitation
Program

Annual Stroke
Center
Continuing
Education

Opioid and Pain
Management

National
Institutes of
Health Stroke
Scale

Basics of
Electrocardiography